
Pandemic Case
Dr.Zhong xiaoling Case report (Corona virus and Hyperbaric Therapy)
Effect of hyperbaric oxygen therapy on the correction of hypoxia in severe COVID-19 patients:
A case report
Zhong xiaoling, tao xiaolan, tang yanchao, Chen ruiyong
China journal of maritime medicine and high-pressure medicine, 2020, 27: network prepublication.
The following contents are protected, shall not be reproduced without authorization, offenders will be corrected!
Progressive hypoxemia is the focus and difficulty of the supportive treatment of severe COVID – 19 (Novel Coronavirus Pneumonia (NCP). It is the main indicator of the classification of light, severe and critical type in the diagnosis and treatment scheme of pneumonia infected by a novel coronavirus (hereinafter referred to as the guidelines) promulgated by the national health commission. Oxygen therapy is the main means of NCP supportive treatment. All atmospheric oxygen treatments have been listed in the guidelines, including nasal catheters, masks, noninvasive and invasive mechanical ventilation, and extracorporeal oxygenation (ECMO) [1]. However, the application of hyperbaric oxygen therapy (HBOT) has not been reported. HBOT inhales 100% oxygen at a pressure of more than one atmosphere to cure diseases [2]. It is the most effective oxygen therapy method known. However, there has been no report on the use of HBOT in the correction of NCP hypoxemia. In a case of severe NCP in wuhan Yangtze river shipping general hospital, atmospheric pressure and high flow oxygen supply were unable to control the continuous decrease of blood oxygen saturation. Based on the analysis of HBOT principle, HBOT is tried for the first time. It was found that the effect of HBOT in the treatment of progressive severe hypoxemia was very obvious. Now the case is reported in detail as follows.
Case data
HBOT program
Results analysis
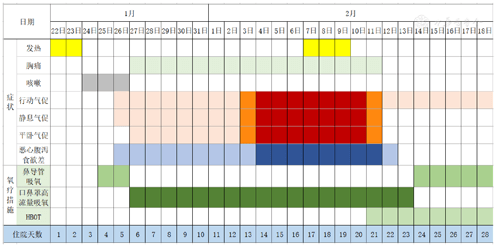
1-Clinical manifestations:
As shown in FIG. 1, the patient still felt dyspnea and chest pain after high flow oxygen inhalation in the supine position before treatment, accompanied by obvious gastrointestinal symptoms. After the first HBOT, dyspnea, chest pain and gastrointestinal symptoms were significantly improved. After the second treatment, the gastrointestinal symptoms basically disappeared. After the fourth treatment, oxygen was given by nasal catheter daily, but the chief complaint of dyspnea after the operation remained. At the time of writing, HBOT patients were continuing the routine HBOT treatment once a day.
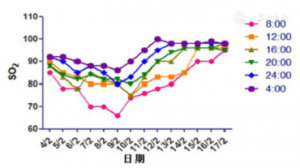
2- Monitoring results of finger pulse SO2:
When the patient was admitted to the hospital, his general condition was ok. After receiving active medication, his respiratory symptoms did not relieve. As can be seen from figure 2, SO2 in patients had the lowest rise in the morning and the highest rise at night. The highest value on day 13 (February 4) was 92%, which was classified as severe according to the medical guidelines. On day 19 (February 9), the lowest SO2 was 66% and the highest SO2 was 86% under the condition of oxygen mask, presenting respiratory distress. Mechanical ventilation support has been recommended, which can be diagnosed as critical illness.
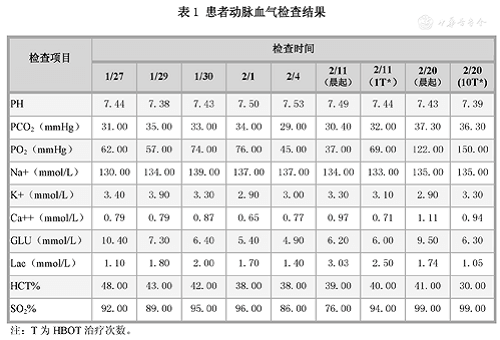
3-Arterial blood gas analysis results:
Due to various reasons, the patient did not reexamine the blood gas after the first treatment except the blood gas. As shown in table 1, the partial oxygen pressure (PO2) before HBOT decreased progressively, which was consistent with the chief complaint and symptoms of dyspnea of the patient. Before the first HBOT (on the 19th day of admission), it was 37mmHg. Reexamination on the day after treatment has been restored to 69mmHg.
4-Hematological examination results:
Due to various reasons, some hematology was not reviewed after treatment. Only before and after comparisons are provided here. As shown in table 2, the lymphocyte count and lymphocyte percentage were consistent with the clinical manifestations and decreased significantly before treatment. Review results after 2 treatments (12 February) showed a significant rebound.
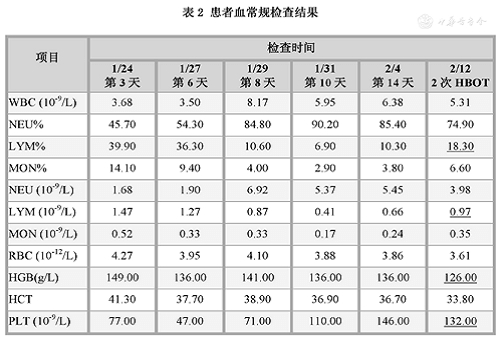
Table 2 Results of blood routine examination
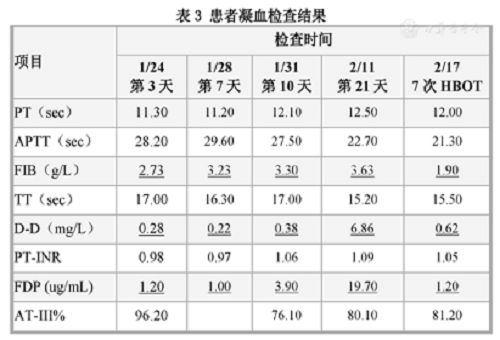
The results of coagulation function test are shown in table 3. Fibrinogen (FIB) was significantly increased on the 7th day after admission (January 28), fibrinogen degradation product (FDP) was significantly increased on the 10th day, and d-dimer (d-d) was further found to be significantly increased on the morning blood test on the 21st day. HBOT was started on the same day. After 7 treatments, FIB, d-d and FDP were significantly reduced, lymphocyte count and albumin were significantly increased, and total bilirubin and direct bilirubin returned to the normal range.
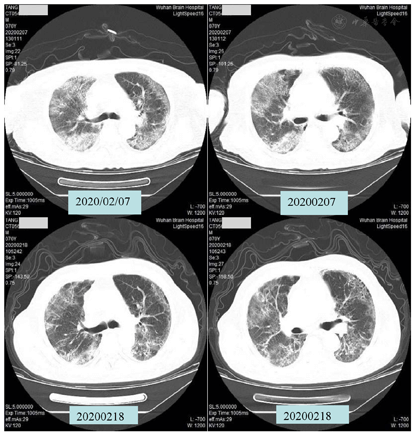
5-CT scan results:
As shown in figure 5, chest CT scan of the patient on February 7 showed multiple specular soft tissue density shadows in both lungs, smooth trachea, thickened vascular texture in both lungs, and multiple flaky high-density shadows in both lungs. The severity of double lung infection was compared with the imaging results on February 3. On February 18, chest CT was re-examined after 8 HBOT sessions, and multiple soft tissue density shadows and flaky high density shadows in both lungs were reduced, but still significant.
Discuss
The course of this case was characterized by persistent and progressive hypoxemia and pulmonary pathological changes. The lung is the main target organ of a novel coronavirus. Pneumonia is a major disease manifestation of a novel coronavirus infectious disease (COVID-19).Diffuse inflammatory changes and hypoxemia in lung tissue are the main clinical features of NCP. Huang et al. reported 41 NCP patients, 12 of whom had acute respiratory distress syndrome (ARDS) complications were ICU care, suggesting that progressive hypoxemia is an important pathological feature of NCP. Of the 27 patients treated with nasal catheter ventilation alone, only 1 (8%) ended up in ICU.However, 62% of patients who rose to require nasal catheter high flow oxygen or noninvasive mechanical ventilation eventually developed into critical care units (ICU) [3]. Chen NS et al reported a similar situation in the investigation of 99 cases of fluid diseases [4]. Hypoxemia is also one of the main causes of death of NCP. The NCP clinical guidelines also use the degree of hypoxemia as the main indicator of NCP clinical classification of light, severe and critical. The radiographic examination of this patient showed that the pulmonary parenchymal lesions were dominant and the respiratory tract was unobstructed. The results of arterial blood gas analysis showed that the PH value was not acidic but alkaline, suggesting that the damage of lung function was mainly caused by the gas exchange function. As a routine procedure, oxygen was administered through a nasal catheter at admission. However, with the development of lung histopathology, SO2 continued to decrease. Further conversion to oxygen mask did not reverse the continuous decline of SO2. The above results suggested that the existing atmospheric oxygen therapy could not meet the needs of the correction of hypoxemia associated with the pathological progress of lung tissues.
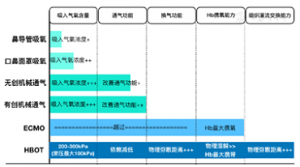
Hypoxemia is a decrease in blood oxygen levels, while hypoxia is a lack of oxygen in a tissue or organ or throughout the body. Hypoxemia is the cause of hypoxia, but not the only one. The ultimate in atmospheric oxygen therapy is ECMO. In theory, the application of ECMO can solve the pathogenesis of hypoxemia in patients. However, the clinical application of NCP in critical cases has limited effect, mainly because of the presence of concurrent multi-organ failure. For the lung as the main target organ of NCP, resulting in multiple organ failure such as systemic dysfunction, in addition to the role of virus and immune response, it is not excluded to be related to the persistence of universal hypoxia of systemic tissues and organs. From the air environment to the cells of the tissues and organs, the oxygen transport amount is affected by the oxygen partial pressure of respiratory gases, lung ventilation function, ventilation function (including the role of air and blood barrier and ventilation/perfusion ratio in gas exchange), blood carrying capacity, and tissue hemoperfusion. The difference in efficacy of existing oxygen therapy methods is related to their ability to intervene in these five steps (figure 6). The clinical selection of oxygen therapy should fully consider the influence of disease on each link and the pertinence of oxygen therapy.
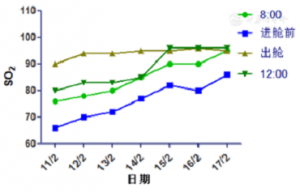
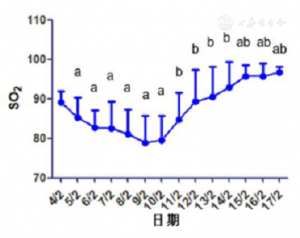
Oxygen debt (also known as exercise excess oxygen consumption) is the difference between oxygen demand and actual oxygen supply, and is commonly used in sports medicine [5]. The fever and strong immune response caused by virus infection will inevitably lead to the increase of metabolic rate and oxygen demand. At the same time, however, the persistent hypoxemia caused by lung histopathology of NCP reduces the oxygen supply of the lungs and lungs to the tissues and organs of the whole body. Therefore, when the NCP disease develops to a certain extent, there must be a gap between oxygen demand and oxygen supply, which can also be understood as a special “oxygen debt”. Studies have found that under certain intensity of exercise load, preexisting lung diseases can lead to hypoxemia [6]. In this case, the SO2 before HBOT entered the cabin was significantly lower than that before under the condition of oxygen inhalation in the ward mask (at 08:00), which was caused by the fact that the patient could not absorb oxygen and increased a certain amount of activity during the process from the ward to the HBOT department. As a result, the oxygen intake decreased and the consumption increased, SO2 decreased. This phenomenon suggested that pathological changes in the lungs resulted in a serious imbalance between oxygen demand and oxygen supply in the patient. Arterial blood gas analysis before the first entry of HBOT on February 11 suggested that the blood lactic acid content was significantly increased (3.03mmol/L), suggesting that the patient was in a state of severe anaerobic metabolism.
HBOT based on gas physics characteristic, through the great increase in oxygen partial pressure, reach the cardiopulmonary function in the same condition, the increase of alveolar oxygen partial pressure, increase the blood oxygen tension, increase effective diffusion radius of tissue oxygen, increase oxygen transport capacity, so as to achieve correct hypoxia (1) valid thoroughly at the same time, improve the acidosis, and organize the cell vitality, enhance (2) after the reoxygenation of capillary endothelial cells, the capillary function can be restored and the exudation and edema caused by hypoxia can be blocked. (3) increase the effective diffusion radius of tissue oxygen, correct tissue hypoxia and increase tissue oxygen reserve [2]. The blood gas analysis results of this patient after the first time HBOT went out of the cabin showed that PO2 increased from 37.0mmHg before entering the cabin to 69.0mmHg, showing a good effect of HBOT correction, but there was an obvious gap with the normal value, and SO2 only increased to 90%. This state before entering the cabin can best reflect the degree of hypoxia of the patient’s systemic tissues and organs. The ultimate goal of clinical oxygen therapy is to solve the hypoxia state of the body. This result suggested that the accumulation of “oxygen debt” in the early stage of the patient exceeded the ability of one HBOT to correct, which further reflected the imbalance of oxygen demand and oxygen supply in the patient’s body.
After the patient left the capsule for 90 minutes (at 12:00), the oxygen saturation of the patient significantly decreased, indicating that the tissue oxygen reserve increased by the physical dissolution of HBOT was exhausted in a very short time. On the whole, however, the daily mean SO2 of HBOT patients increased steadily. Can’t use HBOT residual oxygen explanation, the possible mechanism on the one hand is to provide the body’s aerobic HBOT intermittent (before metabolism of anaerobic – aerobic metabolism in the treatment after – treatment of anaerobic metabolism), greatly improved the body tissue tolerance ability of anaerobic metabolism, mechanism of similar HBOT intermittent oxygen oxygen toxicity tolerance of [2]. In addition, for example, the significant increase of d-dimer, plasminogen and TDP in the hematological indicators of this patient suggested that the patient had existed a certain degree of disseminated intravascular coagulation (DIC) prior to HBOT, which can be secondary to viral infection. There were peripheral hemodynamic changes and perfusion disorders. The change of coagulation index in this patient also suggested the obvious role of HBOT in improving terminal circulation and improving oxygen supply to tissues. Whether DIC combined with persistent hypoxemia leads to ischemic loss and tissue edema of capillary endothelial cells in the peripheral circulation and whether it is a common phenomenon in patients with severe NCP requires more clinical studies and observations.
In this case, due to the lack of medical care in the cabin, oxygen was inhaled for 95min from the beginning of pressurization to the end of decompression. Oxygen poisoning has always been an important problem for many hyperbaric oxygen clinicians in the application of HBOT. The human body is adapted to the environment of 20kPa oxygen partial pressure under atmospheric air, and it will inevitably have an impact when exposed to HBOT’s high pressure oxygen. Due to the necessity of breathing the mixed gas or oxygen with high pressure oxygen during diving, the diving program was designed by limiting the exposure dose of high pressure oxygen to avoid large lung type oxygen poisoning injury [2]. The high oxygen exposure dose of conventional HBOT is about 150 UPTD. In this case, the exposure dose was 216 UPTD, but still much less than 615 UPTD. This dose represents a reduction in lung capacity of approximately 1%, the safe limit for conventional high pressure oxygen exposure. Therefore, the patient’s HBOT did not have to worry about the risk of pulmonary oxygen poisoning.
In this case, CT reexamination after 8 HBOT showed that although the pulmonary lesions of the patient were significantly improved, the lesions were still obvious. However, the patient’s SO2 remained in the normal range under the condition of oxygen inhalation by nasal catheter. Separation phenomenon in this lung pathological changes and SO2, prompt HBOT although not directly to clear effect to the disease (virus), but it provides powerful oxygen cure, as the direct cause of lung tissue pathology may lead to continuous hypoxemia, especially the state of the oxygen to body tissues and organs of oxygen debt continues to accumulate, and its important oxygen consumption of tissues and organs of the secondary injury, keep the function of the body is relatively good state, for the body against infection systemic function provides a good foundation.
To sum up, according to the pathological characteristics of NCP, HBOT has a clear mechanism of excellent action different from atmospheric oxygen therapy. Conventional HBOT has been widely used in clinical practice for decades and has a strong therapeutic capacity. On the premise of solving the transfer process sensing control, large-scale treatment of NCP patients can fundamentally solve the problem of supporting treatment of progressive hypoxia that cannot be contained by current atmospheric pressure oxygen therapy, so as to achieve the expected effect of reducing the critical disease rate and mortality. From the changes in the clinical manifestations and examination results of this patient, it can be seen that 1 HBOT can significantly improve the severe and critical NCP patients whose daily average SO2 is still lower than 80% under the condition of atmospheric pressure oronasal mask and high flow oxygen absorption, and 4 HBOT can basically correct the persistent hypoxemia in critically critical patients. According to the existing critical disease NCP stock in wuhan, in the use of clinical HBOT, measures and practices of combining HBOT with atmospheric oxygen therapy can be further explored to comprehensively improve the treatment efficiency of large Numbers of patients.
Reference
[1] national health commission, state administration of traditional Chinese medicine. Will be coronavirus pneumonia diagnosis and treatment scheme (trial version 5) [S/OL]. (2020-02-04) [2020-02-17].http://www.gov.cn/zhengce/zhengceku/2020-02/05/5474791/files/de44557832ad4be1929091dcbcfca891.pdf.
[2] gong jinhan, Ed. Diving medicine [M]. Beijing: people’s military medical publishing house, 1985:550-561
[3] HuangCL WangYM, LiXW, et al. The Clinical features of patients infected with 2019 will be coronavirus in Wuhan, China [J]. Lancet, 2020395:497-506. The DOI: https://doi.org/10.1016/S0140-6736 (20), 30183-5.
[4] ChenNS ZhouM, DongX, et al. Epidemiological and clinical characteristics of 99 cases of 2019 will be coronavirus root in Wuhan, China: A descriptive study [J]. Lancet, 2020395, 507-513.doi:https://doi.org/10.1016/s0140-6736 (20), 30211-7.
[5] Wang J, wang h, zhu z x. research progress of classical oxygen debt theory [J]. Applied psychology, 1997 (02) : 55-57. (in Chinese)
[6] hopkinssr. Exercise induced arterial hypoxemia: the role of promise-induced inequality and pulmonary diffusion limitation[J]. Adv Exp Med Biol, 2006,588 :17-30.DOI:10.1007/978-0-387-34817-9_3.